
Why is the pelvic floor important?
Your pelvic floor is made up of a collection of muscles, ligaments, bones, and connective tissue. All of these are beautifully interlaced in the hip, lower abdomen and low back which is why we look at and work on mobilizing and strengthening all of these areas and not just the pelvic floor! Yes, we are taking a deep dive into the pelvic floor but that’s because it’s usually the part that we don’t explore.
When the pelvis is aligned, moving and strong, all other areas of the body can move more freely from a solid foundation. Let's talk about why the pelvic floor is important.
Support & Stability
The pelvic floor acts as a hammock for our pelvic organs (bladder, uterus, rectum) and helps keep everything in its place. If our hammock is overly stretched then it can create tension throughout our system and cause pain or it can cause the muscles to weaken. If our hammock is too loose, then the organs may not have enough support to keep them up and in the body.
Sphincter
We have two sphincters made of muscles - one around the bladder and one around the rectum and help with controlling the flow of urine and feces. Think of the sphincters as hose valves- when they are contracted they keep water (err..poop and pee) inside. When they become loose or relax, they allow the pee and poop to freely flow. These muscles contract to help prevent leakage and relax to allow the free flow of urine and easy bowel movements.
POSTURE
The pelvic floor muscles work with the diaphragm, abdominal muscles and back muscles to stabilize the core. The pelvic floor is basically the bottom of a pop can…when the can is properly pressurized it doesn’t leak and is a nice and strong and can withhold a lot of pressure. If there is a hole in the bottom or top or the can becomes indented, then the entire system loses support.
Sexual
We can thank the pelvic floor muscles for the ability to have sexual pleasure as the muscles help increase blood flow to that area. This increased blood flow means increased hormones, increased lubrication, increased arousal and easier pain-free penetration. The muscles of the pelvic floor also surround the clitoris (more on this later) and help increase stimulation so you can orgasm.
Sump-Pump
The muscles of the pelvic floor work to bring blood and lymph in and out of the pelvis. When we lose the sump-pump ability it increases our chance of swelling and pelvic congestion and can cause the muscles and nerves to be irritated. Our nerves LOVE to not have swelling and to be able to fire freely and the constant movement of the pelvic floor allows just that to reduce swelling and congestion down there.

What Exactly is “Down There”?
“It’s ALL connected” is one of my favorite sayings and that’s because the pelvic floor really is connected to pretty much everything. Do you know the song “Dem Bones”?
The “Knee bone connected to the thigh bone. Thigh bone connected to the hip bone. Hip bone connected to the back bone. Back bone connected to the shoulder bone…”
Well, it’s the perfect song for understanding how the body works. Starting at the foot and ending at the head, the bones (and muscles and all of the other juicy stuff in between) really is connected. Naturally we’re going to focus on the area between the belly button and the thigh for this program but I think it’s important we look at and understand how things like our breathing can directly and indirectly affect our pelvic floors!
If you’re thinking, “why would I want or need to know anatomy?” then I’m actually going to ask you a question first. Where is your shoulder? Your toes? If you stubbed your toe on the edge of the bed, could you tell me which one you hurt? For a lot of us, we don’t think twice about anatomy of the body. It’s just a body part…until it comes to the pelvic floor and then it suddenly becomes “weird”. But here’s the catch — when our shoulders or toes hurt we are able to identify where the pain is coming from because we acknowledge that it exists. By putting the pelvic floor in a box never to be opened, we can actually create little areas of our body that we don’t connect with physically or emotionally and it can delay healing. By connecting with our body, even through a little bit of anatomy, we can better understand what’s going on down there.
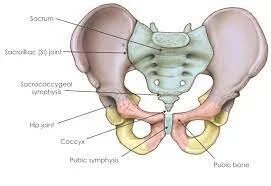
The Back of the Pelvis
SACRUM (and COCCYX)
The sacrum is one of the most important body parts when it comes to the baby making it's way Earth-side. The sacrum literally expands backwards and "opens the back" allowing the baby to better engage and rotate during the second stage of labor. The ability of the sacrum to freely move in labor is one large part of helping the baby engage and emerge from the pelvis because it opens the pelvic outlet (where the baby emerges from the pelvis to the outside world) from front-to-back.
*I'd love for you to visit the North Dallas Doula Association Facebook page from 2019 for a beautiful picture of The Rhombus of Michaelis. It is in the shape of a kite and includes the three lower lumbar vertebrae, the sacrum and the long ligament that reaches down from the base of the skull to the sacrum. The Rhombus of Michaelis is a NORMAL and physiological movement of the spine that quite literally opens the pelvis as it moves backwards to create the maximum amount of space to allow the baby to turn it's shoulders.
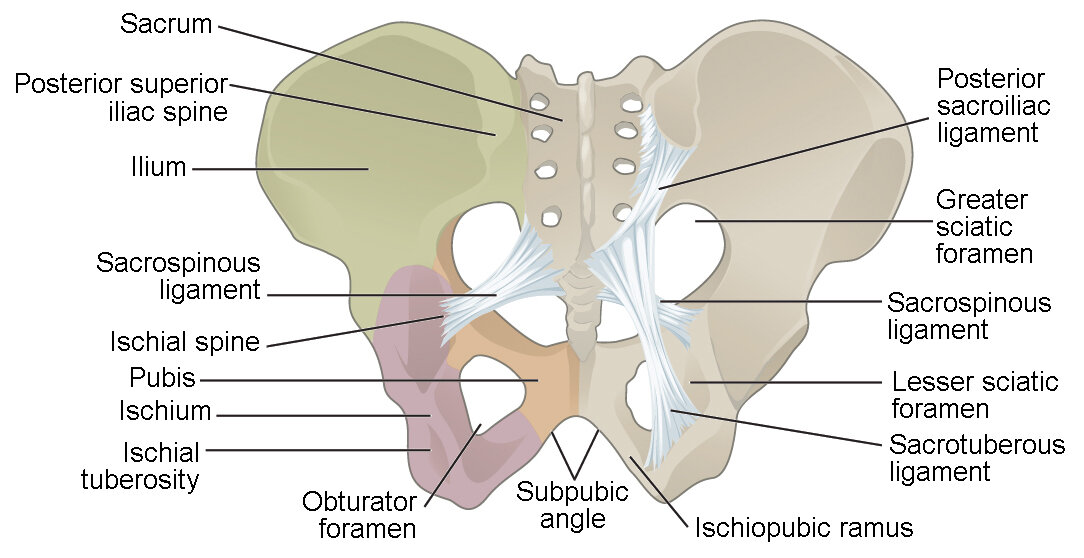
POSTERIOR SUPERIOR ILIAC SPINE (PSIS)
Have you ever felt your low back and wondered what those bony little knobs are back there? Those knobs are your PSIS. Knowing this location will come in handy in the late stages of labor as it is one of the areas you can apply pressure to help ease pain!
ISCHIAL TUBEROSITY
These are often called the "sitz bones" as they are at the very bottom part of the pelvis/butt. If you put your hand at the bottom of your butt, you will feel two pointy bones— these are your ischial tuberosities. These bones are super important during the expulsion phase of labor as they can open side-to-side and make the pelvic outlet (where the baby comes out of) bigger!
The front of the Pelvis
ANTERIOR SUPERIOR ILIAC SPINE (ASIS)
Place your hands on the front of your hips and feel the bony part that tends to stick out the most. These are your ASIS.
PUBIC BONES & PUBIC SYMPHYSIS
The pubic bones are the bony parts at the upper portion of the vulva. The two pubic bones are connected by a cartilage called the pubic symphysis. These are important because they attach to a lot of muscles and ligaments and provide support to the low back, groin and hips. During pregnancy a lot of people have heard about the dreaded lightning crotch (more on that later) and this is where that pain comes from. Although it may be painful, I want you to know that this joint can safely expand almost 3/4 of an inch during labor to help make space for the baby to emerge!
HIP JOINT
I told ya it's all connected. ;) The hip joint that you see is where the femur (your leg) connects to your pelvis. The position of legs directly affects how your pelvis moves and during labor and delivery, how you move your hips can actually help open the pelvis!
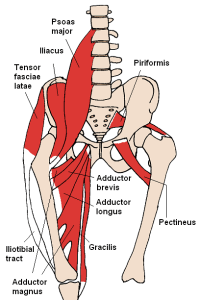
The Pelvic Hammock


First, let’s look at the picture on the left. I’m not going to break down the fine details of the muscles for you. What I want you to take away from this picture is just how many muscles there actually are! Your pelvic floor isn’t one tiny muscle that is holding on by a string ready to break at any moment. It is an amazing collection of interwinding muscles and ligaments that work together to create this strong, stable, resilient base of support. It’s a collection of muscles that when one area is weak, another area can step up and fill it’s spot by becoming even stronger.
I used to refer to the pelvic floor as a bowl but recently I switched to the phrase pelvic hammock. Why am I telling you this? Well, because it’s important. If I have a bowl of hot soup, I’m going to support it with both hands. I’m going to move gingerly in order to not spill it over. A hammock is more resilient. It can tugged and pulled in one direction or a little loose on one side and still be strong and stable. It is made for movement - for rocking back and forth, for a child jumping into it without it breaking. A hammock, just like our pelvic floor, is able to adapt to what we do with it.
From Head-to-Toes with the Pelvis In Between
By Beth ohara (Own work) via Wikimedia Commons

These are two beautiful pictures of the muscles the mostly attach on the front of the pelvis. I hope you can take a moment and admire these beautiful interlacing connections. Often times when people think “pelvic floor” it is a separate unit but that isn’t the case at all—the pelvis connects the hips, the thigh, the low back and the abdomen. I like to think of the pelvic floor as the chains on a bike. When the chain is connected and functioning optimally, the rest of the bike is likely to move optimally. When the chain is stuck or needs a little oil or needs tightened, the bike probably isn’t riding as smoothly as we would like. By correcting the chain (pelvic floor), we can make the entire bike (body) function better.
Fun fact, when our feet are dorsiflexed (toes are pointing toward the head), it naturally activates the pelvic floor. When our toes are pointed away from our head, it naturally relaxes the pelvic floor. This is a beautiful reminder that you can strengthen (or relax) your pelvic floor simply by changing your foot position!
The Pelvic Floor, Diaphragm & Jaw Connection
This may be my favorite connection of all — the jaw, diaphragm and pelvic floor connection. Every time we inhale our pelvic floor naturally lengthens and elongates and every single time we exhale the pelvic floor gently contracts and lifts. A random fact is that when we take a deep inhale, the kidney moves down almost half an inch! The pelvic floor doesn’t move that much because of all of the bony attachments but just think about how much pelvic floor movement (both relaxation and strength) we can get every day by simply breathing. It’s like doing 22,000 reps of an exercise every single day…just because you remembered to breathe.
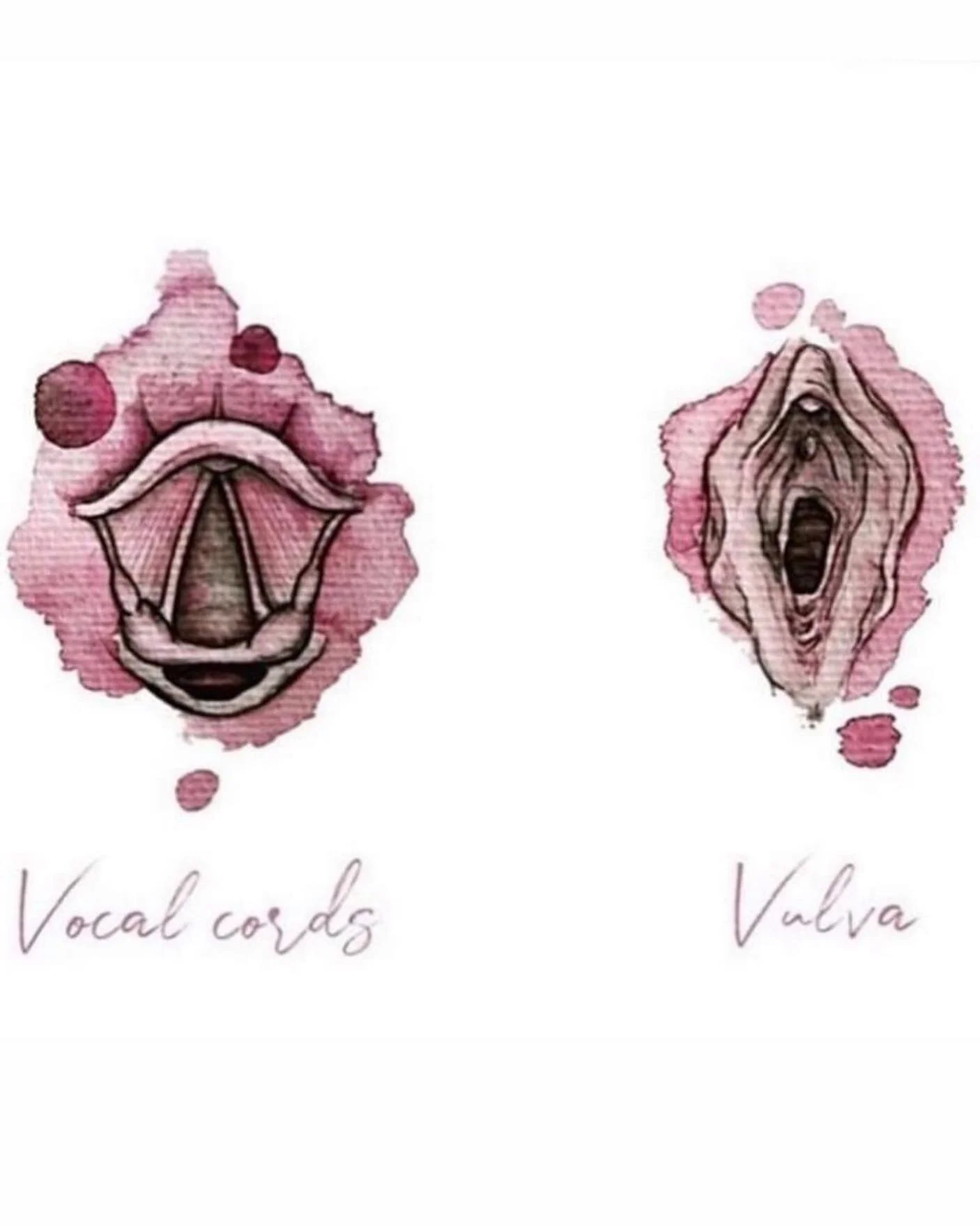
The jaw and pelvic floor connection is also a masterpiece in and of itself.
Starting at the Toes and Working Up
These are two beautiful pictures of the muscles the mostly attach on the front of the pelvis. I hope you can take a moment and admire these beautiful interlacing connections. Often times when people think “pelvic floor” it is a separate unit but that isn’t the case at all—the pelvis connects the hips, the thigh, the low back and the abdomen. I like to think of the pelvic floor as the chains on a bike. When the chain is connected and functioning optimally, the rest of the bike is likely to move optimally. When the chain is stuck or needs a little oil or needs tightened, the bike probably isn’t riding as smoothly as we would like. By correcting the chain (pelvic floor), we can make the entire bike (body) function better.
Fun fact, when our feet are dorsiflexed (toes are pointing toward the head), it naturally activates the pelvic floor. When our toes are pointed away from our head, it naturally relaxes the pelvic floor. This is a beautiful reminder that you can strengthen (or relax) your pelvic floor simply by changing your foot position!
The Pelvic Floor, Diaphragm & Jaw Connection
This may be my favorite connection of all — the jaw, diaphragm and pelvic floor connection. Every time we inhale our pelvic floor naturally lengthens and elongates and every single time we exhale the pelvic floor gently contracts and lifts. A random fact is that when we take a deep inhale, the kidney moves down almost half an inch! The pelvic floor doesn’t move that much because of all of the bony attachments but just think about how much pelvic floor movement (both relaxation and strength) we can get every day by simply breathing. It’s like doing 22,000 reps of an exercise every single day...just because you remembered to breathe.
The jaw and pelvic floor connection is also a masterpiece in and of itself. When we look at the vocal cords and pelvic floor (or vocal cords and vulva), we can see a resemblance in how they are structured. This connection actually started when you were in-utero! As the female embryo develops the vocal cords and ovaries start as one unit and later split as the baby develops.
Aside from the embryological connection, I frequently have people complain of constipation when they get stressed or anxious. Along with not having regular bowel movements these people are usually jaw clinchers or teeth grinders. That’s because the jaw/tongue and the pelvic floor are interlaced from a nerve connection. The Vagus nerve is a large, beautiful nerve that connects the brain and the sacral plexus (head to butt). This nerve is in charge of our parasympathetic response - rest, digest. It’s really common to hold both the jaw and pelvic floor tight when we are in a fight-or-flight mode so by working on one we can help the other!
Don't take my word for it. Instead, take a deep breath in and then exhale and say "ahhhhhhhhhh" and feel where you notice the sound resonate. Do you feel the vibration in your throat? In your tummy? In your pelvic floor? Next try the saying "eeekkkkk" and do it in a higher pitch...you should notice that your pelvic floor naturally lifts. Finally, try the same thing in a low tone or slow moan saying "ahhhhhh". You probably notice that your pelvic floor naturally drops down a little and relaxes.
If you have trouble noticing these connections, you can also stick your thumb just behind your front top teeth, put your tongue on your finger and suck really hard (like a baby nursing). Notice what your pelvic floor does. As you suck, your pelvic floor should naturally lift!
One reason I wanted to highlight these connections is because sometimes it might seem like you aren't "working the pelvic floor". In reality, working away from the pelvic floor can help the pelvic floor move more freely, be better stabilized and connected to the rest of the body.


Connecting to Your Pelvis
When was the last time you checked in on your pelvic floor? This audio does just that and lets you tap into what is going on down there. You can think of it as progressive relaxation for the downstairs. The goal is to help you connect to, listen to and appreciate what the pelvic floor is telling you.
Pelvic Bowl Visualization & Sweep
Each of us are unique so this may or may not be up your alley and that’s okay. The goal here is to start connecting with the pelvic floor emotionally and mentally. This meditation was adapted from the amazing Lynn Shulte of the Institute of Birth Healing.
Written Meditation:
Get comfy in your chair with your feet grounded on the floor. Take a deep breath in and as you exhale bring your awareness to your pelvic floor. Feel your chair wrap around your butt as you sink into the chair. Feel the energy of your feet, connecting with the ground beneath you. Now, feel the energy of your feet wrap upwards towards the pelvic space, wrapping around the pelvic bowl and hugging it. Visualize the energy expand into your abdomen and chest. Let the energy expand up into your head and allow your head to open to the world around you. Bring the energy that surrounds you down and let it wrap around your shoulders and chest, and rest into your abdomen and pelvis. Next, visualize your pelvic energizing bowl - just as the energy you connected with through from your feet and the area around you can be large or small so can your pelvic bowl energy.
First, be present with the bowl. Don’t try to change anything but simply accept your pelvis bowl as it currently is. Take note of the shape of your bowl. Color. Texture. Size. Notice how it sits. Is it level or tilted to one side? How tall or short are the walls? Are there any dents or cracks? Do you feel drawn to a certain part of the pelvis?
Now we are going to sweep the pelvis. The pelvis can be an energy powerhouse - it can store unprocessed emotions or events. It We are going to clear the pelvis out of the energy that we currently have permission to clear. Stand on top of the pelvic bowl and visualize the vaginal opening as the drain. Use whatever tool feels most appropriate now - a hose, brush, broom, backhoe, spatula - invite whatever tool you need right now into your space. Slowly move around the pelvic bowl and sweep whatever energy you have been holding onto and release it down the drain.
Do you feel something stuck or resistance? Just let it sit there and be present. Do not force it. Sit and let yourself connect and feel whatever emotions may come without justifying or changing your emotions or your pelvic bowl.
Continue walking around your bowl and sweeping your bowl. Once you are done sweeping, check back in and see if there is anything that has changed or anything that is different.

From Pee to Poop -What is “normal” down there?
All too often when it comes to the pelvic floor we hear the word “normal” thrown around without any reference to what exactly "normal" actually is. So without further ado, here are 10 normal bowel & bladder functions:
1. Going to the toilet 6-8 times in 24hrs: Ideally you will only need to go at most one time overnight and you should be going to the bathroom every 3-4 hours during the day. Please note that you don't want to hold pee for the entire work day or 8-12 hours.
2. Pee for ~8 seconds with a steady and smooth stream (or spell out MISSISSIPPI): Peeing shouldn’t sound like a water faucet trickling or a jet taking off. It also shouldn't take 2 seconds or be an extravaganza that takes a minute. The one exception here is that glorious first morning pee which can take longer!
3. Pee should go straight down: Serious question, have you ever watched where your pee goes? If you look down would it be shooting to the left or right? In case of an emergency, would you be able to "aim" and pee into a bottle or would you pee everywhere?
4. Easily pass a bowel movement with minimal strain daily: Ideally you will have 2-3 bowel movements a day approximately 30 minutes after you eat (that's when your bowels naturally release). This also includes passing gas so you should be able to pass gas without pain, pressure or feeling like you have to squeeze it out. Finally a fun poop fact is that your poop should resemble a snake...long and soft. If your poops look like something a rabbit deposited or is skinny like a pencil or as large as a summer sausage, these can all be signs your pelvic floor needs a little TLC.
5. Having an increase in vaginal discharge: This can also be increased thickness or vaginal discharge at ovulation. A little discharge is normal but you shouldn't find yourself questioning if you constantly have a UTI. During our cycles we have normal changes in discharge and this includes an egg-like mucus at the time of ovulation.
6. No leaking ANY urine at all, under any circumstance: You should be able to laugh, cough, sneeze, run, jump [yes, even on a trampoline] or do double unders if that’s your thing without leaking
7. Control gas or flatulence under any load: Walking farts, qweefing or vaginal farts are a no-go.
8. Pain-free intercourse and no difficulty with penetration: Dare I say that sex should be enjoyable? Heck yea, I will shout that from the roof top. You deserve to have sex and not be in pain!
9. Control the urge to go potty: You should not be sprinting to the bathroom frequently. You should also be able to hear water running without the urge to go. This includes being able to walk around a store and not needing to know where every single restroom is for fear of peeing your pants. You should be able to enter your house without doing the potty dance.
10. Use a tampon/menstrual cup: If you choose to use a cup or tampon you should be able to do so without difficulty, pain or it falling out!
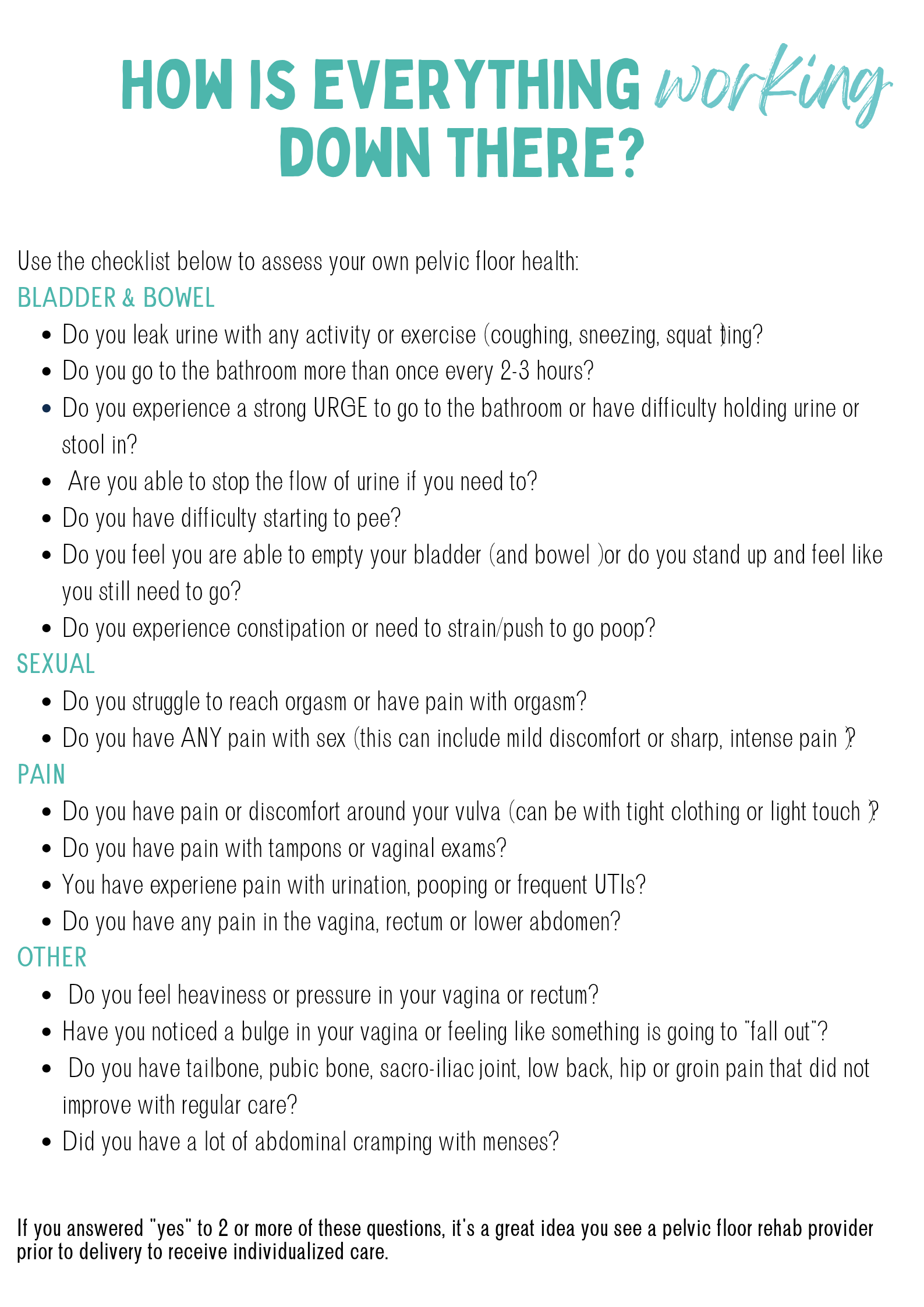
How are things feeling down there?
Often times the pelvic floor is considered taboo but I wish that wasn't the case because it is such an important and powerful part of our body...especially during pregnancy, labor and delivery! In the upcoming sections we are going to do a little self-exploration of down there. You can choose to do this through external evaluation, internal evaluation or feedback. However, until then this is a self-assessment that will help you understand if you are experiencing any pelvic floor symptoms. Some of them may surprise you as being pelvic floor related (hello, constipation and UTIs) while others may simply make you shout, “I knew it”.
Either way, download the document and see just how things are feeling down there to help you determine if you want 1:1 care or if you think you are good to go to navigate this journey on your own.

Incontinence/Leaking
There are a two main types of urinary incontinence - urge and stress incontinence. Urge incontinence is when you have a sudden, strong urge or sensation that you need to pee. This is often noticeable when you pull into the driveway and you notice you have to go RIGHT now. Stress incontinence is leaking with running, coughing, sneezing, laughing, jumping, singing, or simply speaking loudly. If you notice both urge and stress incontinence, then look at improving the urge first!
Are you thinking “what if I leak without physical activity, sneezing, coughing, yelling or with an urge to pee?” This is something that needs to be looked at with a primary care provider as this usually indicates something else may be causing the leaking.
Side note: If you notice frequent urination or urgency that comes and goes it is equally important to rule out infection or medication side effects. Common medications that increase incontinence or urgency are anti-anxiety medications, anti-depressants, ACE inhibitors and NSAIDs (Advil, Motrin).
If I’m leaking or have a prolapse then I need to work on strength, right? Nope. Nada. Definitely not. In order to have an optimally functioning pelvic floor (aka no incontinence) we need the pelvic floor to be mobile, strong and coordinated. That’s why it was important to look at what is actually going on to make sure you aren’t contracting and making it “stronger” when really it needs to be relaxed!
Urge incontinence is usually managed through lifestyle modifications so I included an handout below to help you navigate that. If you are experiencing stress incontinence, this is where a local provider who can help you navigate all of the little functional things that commonly cause incontinence.
A post void dribble is exactly like it sounds - a little bit of urine comes out after you have already used the toilet and then go to stand up. The post void dribble can be caused by a few things discussed in the handout below.
2. Perineal Massage and Scar Tissue Release
Did you know that perineal massage isn’t just for mamas that are expecting? Nope, perineal massage can be used by anyone! The perineum is an amazing area that sometimes gets tight or doesn’t like to move - this could be because of a tight or hypertonic pelvic floor or it could be a side effect of perineal tearing or an episiotomy or other scar tissue. Either way, making sure this tissue is nice and mobile is a great way to make sure the rest of the pelvic floor is able to move freely.
3. Constipation & Rhoids…Oh My!
Constipation and Hemorrhoids are never fun. They are also closely related to a hypertonic or tight pelvic floor. If you find yourself struggling to go daily, working on both your pelvic floor and gut health (see functional medicine provider info below) can help take toilet time from dreadful to uneventful (dare I say, joyful?). I’m not going to make promises for glorious poops but having control over your pelvic floor and having a diet that works for your needs can definitely ease the struggles of constipation and hemorrhoids.
If you have been struggling with constipation for awhile, I highly recommend Dr. Tina Chaney’s Constipation course.
Lubricants 101
I have a weird confession, I love talking lubricants with people. Mainly because I realized how little we actually talk about it (kind of like the pelvic floor). The thing is, the lubricant we use can help nourish our tissues or it can cause irritation. The lubricant we use can help optimize our bodies for conception or it can help act as a contraception. There isn’t one lubricant that is right for everyone at every season of life. That’s why it is important to know what your goals are before deciding the best lube for you right now!
I wish that all lubricants were created equal. Unfortunately that just isn't the case. In all reality, the best type of lubricant depends on your goals! Did you know the best lubricant for moisturizing or doing perineal massage is different than the best lubricant for conception or contraception? This download covers all things lubricant including which products are great for your personal goal at the time.

Kegels are the Snozzberries of the Pelvic Floor
Let's channel one of my favorite childhood movies, Willy Wonka, for a minute. Do you remember the line where Willy Wonka says, "The strawberries taste like strawberries. The snozzberries taste like snozzberries!"? Veruca Salt countered with "Snozzberries? Who ever heard of a snozzberry?" I feel like kegels are the snozzberries of the pelvic floor. Sure, you've probably *heard* of them, but do you really know what a kegel is or what it looks like or even better, what it feels like?
In an ideal world every person would have a consult with a pelvic floor provider who can help them figure out if they need kegels (pelvic floor contractions) or reverse kegels (pelvic floor relaxation). However, I realize not everyone has access or feels comfortable seeing someone. That’s why I created the self-guided assessment - to help you learn your pelvic floor and to make sure they have strength, mobility and coordination. I believe that everyone should have the ability to know what’s going on down there.
I also understand not everyone is comfortable doing a self exam and that's OKAY- don't push yourself to do anything you are uncomfortable with. If at anytime you don't feel comfortable, you have the right to stop for any reason!
The purpose of this self evaluation is to help you learn about what is even down there. Being able to truly visualize and feel what is happening now can help you better connect with your body.
During labor and bowel movements we want the pelvic floor muscles to lengthen (relax) and bulge. By learning about how your body functions down there now, you can have better access and control to the muscles later when you need them. It's just like riding a bike, but instead of a bike we are relaxing our pelvic floors to have a baby or a bowel movement.
When we cough, sneeze or laugh, we want our pelvic floor muscles to quickly respond and fire to lift the pelvic floor. If they are constantly tight or weak, then they aren’t able to create this quick response and can cause leaking.
I’ll be honest, it can feel awkward and hard at the beginning but the more we practice, the better we get until these things become second nature. Let’s start by journaling these emotions.

Grab a pen & paper and write down your thoughts as you work through these next few questions.
When you hear the words "pelvic floor" or "vagina," what thoughts come to your mind? What emotions do you have when you hear these words?
.
.
How does it make you FEEL to hear the word "pelvic floor"? Do you catch yourself taking a deep breath and holding tight down there or do you feel relaxed? Does it make any pain you may be experiencing change? Do you feel icky like you want to crawl out of your skin?
.
.
Have you ever explored down there? Do you feel comfortable with bodily exploration or do you think it is something to only be discussed behind closed doors in a dark room in silence? What are your feelings around it? Do you feel curious, supported, loved, guilty, ashamed, proud?
.
.
Have you ever experienced trauma to your pelvic floor? A previous birth that didn't go the way you visualized, a fall on the butt, an unwanted encounter? How do those memories make you feel? Our bodies hold trauma and can unknowingly cause tightness in response to these.
.
.
Now, think of a time when you felt empowered, supported, loved, energized - what experiences or activities do you have where your pelvic floor was involved and it brought joy? Maybe it's running or dancing, maybe it's swimming or having sex. Focus on those times as you journey through this section. The goal of this section is to help you learn about your pelvic floor. We want to connect with our body now so we can feel confident and trust our body later.
Working Through the “Ick”
You may be thinking, “My mom never said those words to me and then after the puberty talk at school she purposefully made them super cringey. I know it’s important but I have a hard time even saying them myself.” It’s okay that it feels really hard when there is an emotional connection.
One thing that might help is adding the words first. Simply say the words that made you feel uncomfortable. Sit with the discomfort it creates for 2 minutes and see how it feels. And keep doing this. Let yourself feel the cringe/ick and yet move forward. It takes time, practice and healing to change the stories we've been taught.
What’s Going On “Down There” - The Options
When it comes to your vagina you always have options. You always have the ability to do nothing, do a little or do more. My only hope is that you chose the best option for yourself at this moment.
I am including three different ways to evaluate your pelvic floor. The beauty of this is that YOU get to pick what is most comfortable for your body today. You are more than welcome to try all of these if you feel comfortable with it or you can stick with one or two options for self-evaluation. The three options are:
1) External Evaluation Only - Grab a hand mirror for this one as you will be looking at how your vulva and vagina move without ever touching down there.
2) Internal Evaluation - Find a comfy spot, grab a hand mirror and lubricant and kick back with your feet on the ground and your knees up so you can relax and find out what exactly is going on down there.
3) Biofeedback - Grab an exercise ball, a rolled up towel or a yoga block for this evaluation. This is a beautiful option if you don't feel comfortable with the hand mirror or internal evaluation. Even if you feel comfortable with the internal and external evaluation, this one can be amazing as it helps you better connect with your pelvic floor during daily movements like sitting and can also help you "check-in" with your pelvic floor during more intense exercises.
IS ONE OPTION BETTER THAN THE OTHER?
The BEST option is the one that works for you both physically and mentally. Have you ever watched a child learn and explore? Some kids learn with hands-on techniques and doing it themselves, others learn best by watching someone else or observing what happens, and others learn by exploring what's around them. Connecting with our pelvic floors is no different than a child learning the world around them - it might feel awkward and clunky at first, but once we figure out what works for us, it is smooth moving in the future.
The External Assessment
Congratulations on choosing the external assessment. Go ahead and grab a hand mirror and a comfy spot as we are going to look at how our pelvic floor looks at rest and when we both contract and relax!
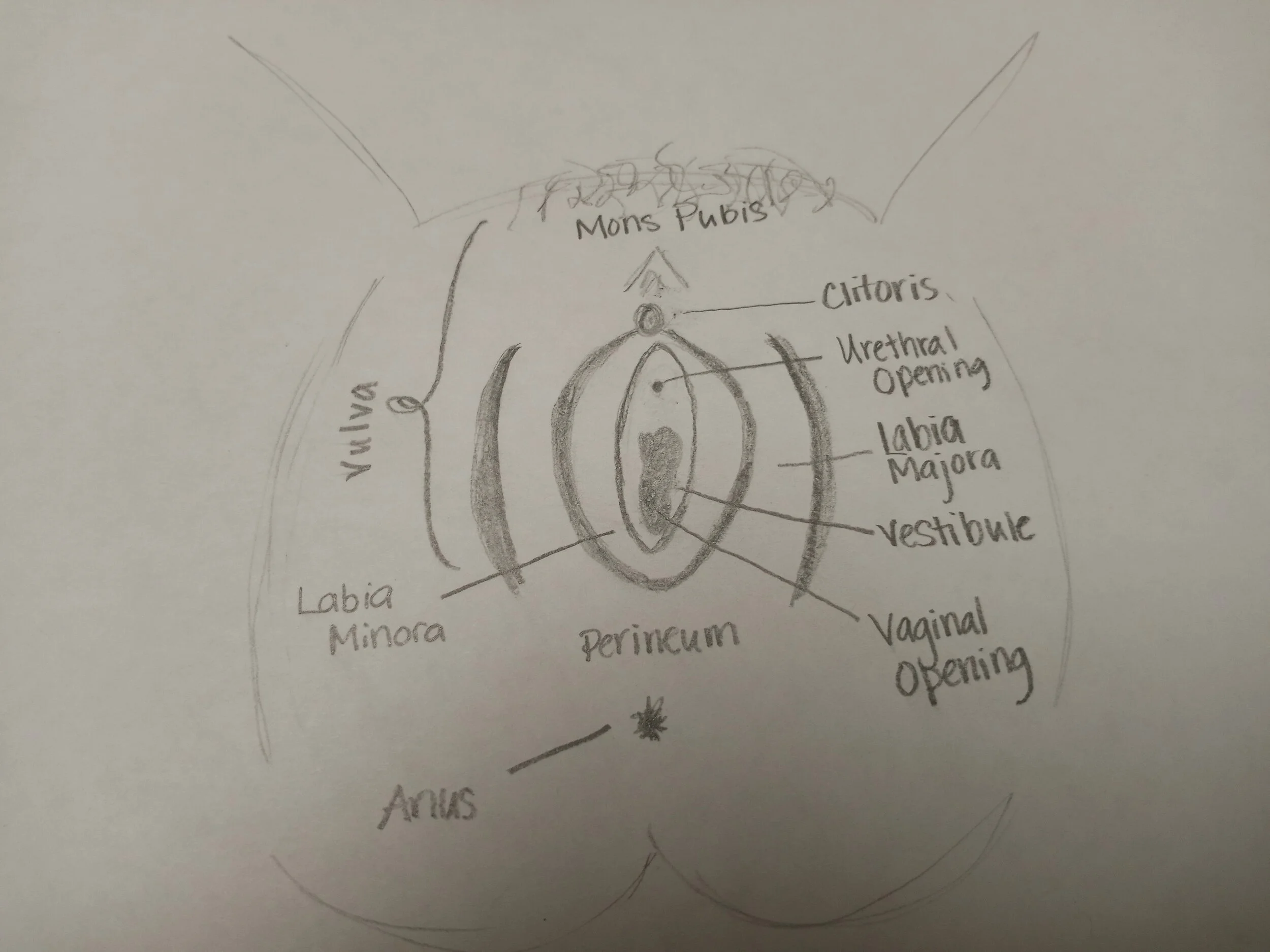
If you are wondering, "does this look normal?" Check out http://www.labialibrary.org.au and see that no two labias are the same!
For the majority of people, what you are looking at is COMPLETELY NORMAL. The only catch is if you notice any whiteness or bright red coloring around the tissue or if the tissue looks shriveled. In these instances it is a great idea to reach out to your provider for a more thorough evaluation.
The Internal Assessment
Next we are going to move on to the internal assessment. Ideally you complete the external assessment first before moving onto this portion as the external assessment can give a lot of detail. Again, you have permission to stop at any time if you feel uncomfortable for any reason.
For this assessment, it’s important to trim your nails, wash your hands, use lubricant to avoid discomfort and grab a hand mirror. If you’ve been experiencing any pain or tenderness, grab a Q-Tip as well. If you prefer gloves, that is also an option!
Feedback Assessment
The beauty of this assessment is that it can be done fully clothed. It also gives us a TON of information because it allows us to connect our minds to our pelvic floors making little check-ins down there make a little more sense. After this assessment you will know how your pelvic floor moves when you are sitting. The thing is, you are almost always moving - sitting. walking, squatting, picking things up (kids, toys, laundry) and putting things down. Sitting still isn't what most of us strive for - we want to move, we want to play, we want to enjoy life. Luckily, the same things we looked at/felt when we were sitting are what we look for in all of the movements throughout the day!
If you notice that you have tension at the end of the day but only after walking, once you do this assessment it can help you “check-in” down there even when you are walking or sitting or lifting so you have a better understanding of what’s going on throughout daily life. The only thing you need for this evaluation is an exercise ball, a rolled up towel or a yoga block to place under your perineum.
Other times you can check in on your pelvic floor and abdomen include:
Sitting in the chair
Brushing your teeth
Picking your child up from the floor
Washing dishes or doing laundry

From Assessment to Reality - Connecting the Dots for a More Resilient Pelvic Floor
Okay, now that you know what’s going on with your pelvic floor it’s time to figure out what to do with it so you can stop guessing and start taking control of everything down there. In the past few sections we looked at the assessment and what was happening when you took a breath or tried to contract and relax. Now, we’re going to take the guesswork out so you can focus on your needs.
This section will help you better understand what you just saw/felt when doing the self-examination. It will also include things other signs that may indicate you are having difficulty relaxing, contracting or trouble with coordination. You can also have a combination of these things which is why a pelvic health provider is important to figure out what is best for you!
If you're anything like me, you may need a little help relaxing your body...and that includes your pelvic floor! It is really common for Type A mamas that are used to the rush of go-go-going. We tend to clench our jaws, tense our pelvic floors and have a bajillion and one things on our to-do lists. If this sounds like you and your self assessment showed you need to relax down there a bit, this handout is for you.
Did you find that your pelvic floor has two left feet? That when you contract or relax that one area felt different than the other? If so, this handout on coordination will help guide you to improved coordination and pelvic floor function.
Okay, so you did the assessment and found that your pelvic floor could use a little strengthening. You're probably thinking you need to kegel your way to a rocking pelvic floor. And while kegels can help, they also tend to be a little bit of a mystery as people don't know if they are using the correct muscles.
Below you will find a helpful little handout to help you move beyond kegels while also strengthening the pelvic floor.
Prolapse
Prolapse is where one or more organs move from their original position downward in the vaginal canal. These are the most common types of prolapse:
Cystocele: the bladder descend into the front of the vaginal wall
You may notice frequent urination or a strong urge to urinate, incontinence (stress, urge or coital), bulge in the vagina, feeling like you have a tampon stuck (phantom tampon), pressure in lower abdomen, pelvis or low back, frequent UTI
Urethrocele: the urethra (tube that carries urine from bladder to the outside) descends into the front of the vaginal wall
Common symptoms you may experience are vaginal irritation, frequent UTIs, feeling of heaviness or pressure in the vaginal canal (like you're sitting on a golf ball), achiness, difficulty fully emptying bladder, frequent urination
Urethrocystocele: both the bladder and urethra descend
Uterine: uterus shifts downward into vaginal canal
This is commonly noticed when having a bowel movement or sitting on the toilet when you "see something bulging" down there
Vaginal Vault: top of the vagina tips down on itself
This is most common after a hysterectomy and people commonly experience incontinence, increased discharge, heaviness/pressure in vaginal region
Rectocele: the rectum pushes into the back of the vaginal wall
Common symptoms include difficulty having a bowel movement or constipation because the rectocele can create a "u" shaped curve of the colon
You may notice rectal pain, pressure, hemorrhoids or impacted (hard) stool, discomfort during sex or pressure on the vaginal wall coming from behind
Enterocele: the small intestine descends into the area between the colon and posterior wall
This usually occurs with uterine or rectocele prolapse
You may experience low back, pelvic or abdominal pain that is relieved with lying down, constant urge to have a bowel movement (like you always have to fart), pulling sensation in abdomen, pain with sex
Rectal: the rectum descends on itself (it folds outward of the rectum)
For rectal prolapse you will often see the prolapse itself along with experiencing bleeding, hemorrhoids, constipation, rectal pressure, mucus discharge in stool, pressure/bulge in rectal region
PROLAPSE NEXT STEPS
Now that you know the different types of prolapses you're probably thinking, "What if I don't know what is prolapsed?" or "my OB said I have a cystocele but my PT said I have a urethrocele...which is it?" and those are great questions. The first thing I want you to know is that the specific types of prolapse don't play a large role in how you feel! You may be thinking "if I don't know what is prolapsed, how can I help it?" but in the grand scheme of things, it's more important to know if it is the anterior aspect (bladder, uterus, urethra) or the posterior aspect (rectocele, enterocoele) than the actual organ that is prolapsed.
You may be thinking, "Why doesn't it matter?" and that's a completely valid question. We don't do exercises to specifically strengthen the bladder or the uterus or the rectum...instead we focus on strengthening, supporting and mobilizing the muscles, tendons, ligaments, fascia and joints that connect ALL of those structures. By strengthening those supporting structures, we can help improve the bladder AND the uterus AND the rectum. Which is why the diagnosis alone isn't what's important...what's important is how you feel, move and connect with your body.
Prolapse Grading
There are usually three main questions people ask when they first find out they have prolapse. The first is what type of prolapse they have and the second is the grade/ severity. The third question is if they will struggle with prolapse forever.
This section we will focus on two of those three things...the grade and recovery. Below are the four common grades of prolapse.
Grade 1: Greater than 1cm above the vaginal opening
Grade 2: Within 1cm above or below the vaginal opening
Grade 3: Slightly below the vaginal opening
Grade 4: Maximal descent outside vaginal opening
While we could go over the different grades, there are a few things I feel are more important.
1) The severity of prolapse is NOT related to symptoms
Yep, that's right. Even if your bladder or uterus descends a little from where they started, it does not mean you will be symptomatic. On the other side, you can have symptoms and have a "small" or "mild" prolapse. It is both common and normal for someone who has a Grade 2 prolapse to notice symptoms while someone with a Grade 3 prolapse may not have any symptoms only the physical sign of a prolapse.
2) Many believe that a Grade 1/2 prolapse is considered normal.
Not just common, but truly normal. This is important because some level of descent is common as we age and move and doesn't mean there is anything "wrong". Having a prolapse does not mean you are broken...in fact some people don't even know they have a prolapse because they don't have symptoms!
3) Prolapse isn't strictly about the pelvic floor
Often times you hear the word prolapse and immeditely think, "I need to do more kegels" but that simply isn't the case. It's equally about the muscles, ligaments, tendons, joints, fascia, blood flow, hormones, stress resilience, sleep, bowel habits and even your physical and emotional connection with others.
These are important because some level of descent is common as we age and move and doesn't mean there is anything "wrong". Also, simply because you have a descent of the organs does not mean you will have symptoms. The key to managing a prolapse is to have a mobile, stable and coordinated body, including the pelvic floor, core, feet, jaws and everything in between. If you noticed a prolapse, please know that you are not broken.
I would love for you to focus on your resiliency and strength as you move forward. Focusing on what you can do while working to decrease symptoms can help you heal and recover faster.
Why do Prolapse Symptoms Change?
Much like life, prolapse symptoms often ebb and flow. Meaning that some times you'll feel like a rockstar and sometimes you'll feel like you have a rock in your pants. I fully understand this can be frustrating and it's equally important to know it is normal. I invite you to think of those ebbs as a message from your body, asking you to listen in to what it is saying and take action from there.

Why Do Prolapse Symptoms Change?
Much like life, prolapse symptoms often ebb and flow. Meaning that some times you'll feel like a rockstar and sometimes you'll feel like you have a rock in your pants. I fully understand this can be frustrating and it's equally important to know it is normal. I invite you to think of those ebbs as a message from your body, asking you to listen in to what it is saying and take action from there.
Here are a few times you may notice ebbs and flows:
*ILLNESS: If you are sick, your body is naturally under more stress and the goal is to get you better. The body focuses on healing and it will naturally shift hormones to focus on healing and stress recovery over sexual hormones to assist with pelvic floor healing.
If you've been coughing or sneezing a lot, it is not uncommon for the pressure you build due to the cough to go downward. Don't worry we'll talk about this a lot more in the incontinence section! For now, just know if youre recovering from a cough, sneeze or allergies, it is common to experience more epelvic floor symptoms.
*CONSTIPATION, GAS, BLOATING: If you are not going to the bathroom regularly, constantly straining or have gas and bloating, all of these can increase prolapse symptoms. We talked earlier about the importance of the breath in stabilizing the back and pelvic floor. In the instance of constipation or gas, you can think of a balloon being blown up. As you blow it up, it starts to reach its capacity and often times a balloon will simply pop if it has too much pressure. Thankfully we don't truly pop! Instead when we have increased pressure from constipation or bloating it's like trying to blow a balloon up with a child pushing on the other end...as you blow the balloon up, instead of moving outward the pressure has to go elsewhere. In the case of the balloon you'll feel the air shooting sideways or going toward your face. For your body that pressure usually goes in one of three directions- up causing reflux, out causing a diastasis or down irritating a prolapse.
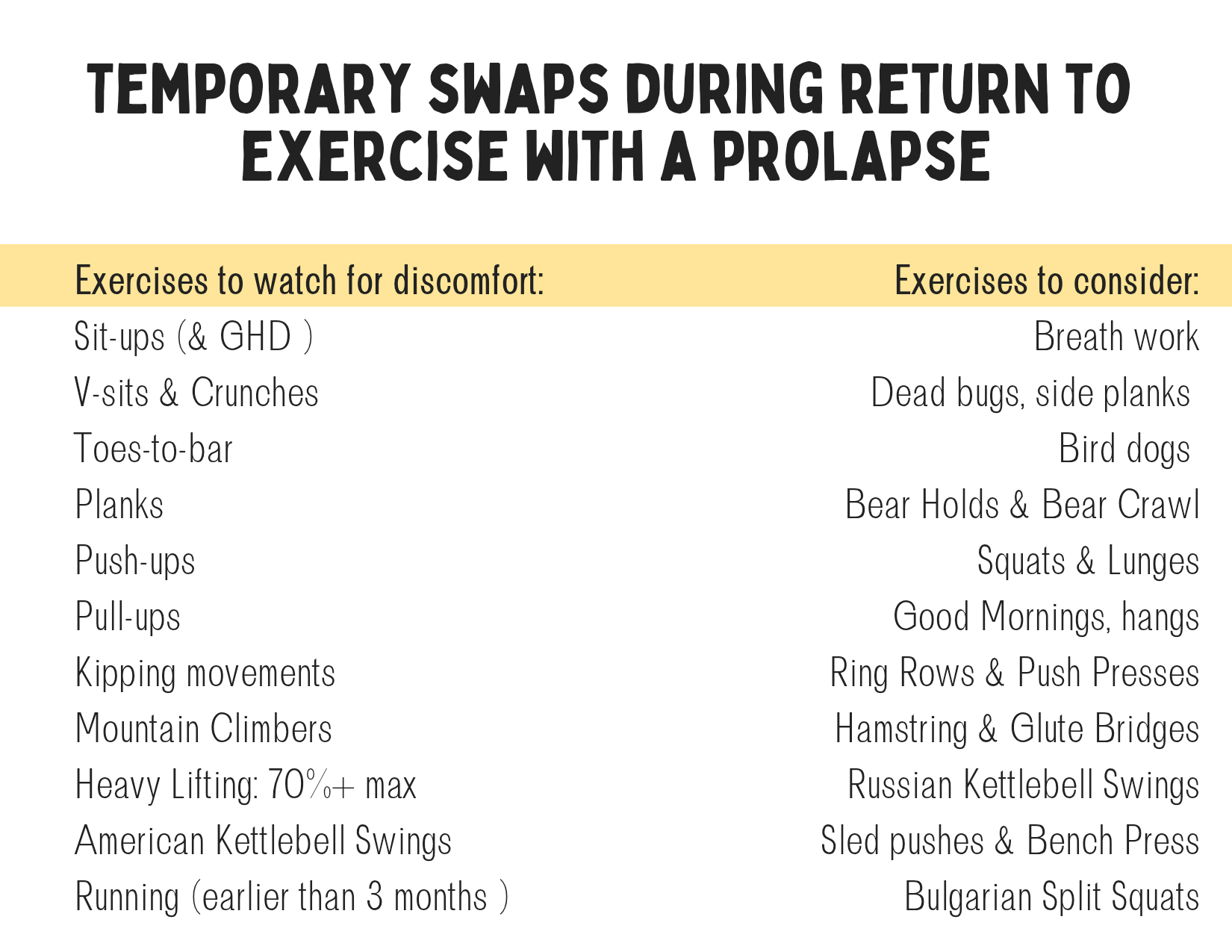
*EXERCISE: This one is definitely tricky because it's not so much about the exercise you do as much as HOW you do it and how much of it you do. A lot of mamas with prolapse can still run 5ks or half-marathons or lift heavy weights or do yoga. The key is to modify the exercises that cause a flare for YOU, understand the cues YOUR body is giving you and to test the boundaries so you can continue to progress rather than being stuck in a plateau. You may need to decrease the load (or distance) temporarily but the goal is to improve, grow and increase that load so you can be more resilient and strong.
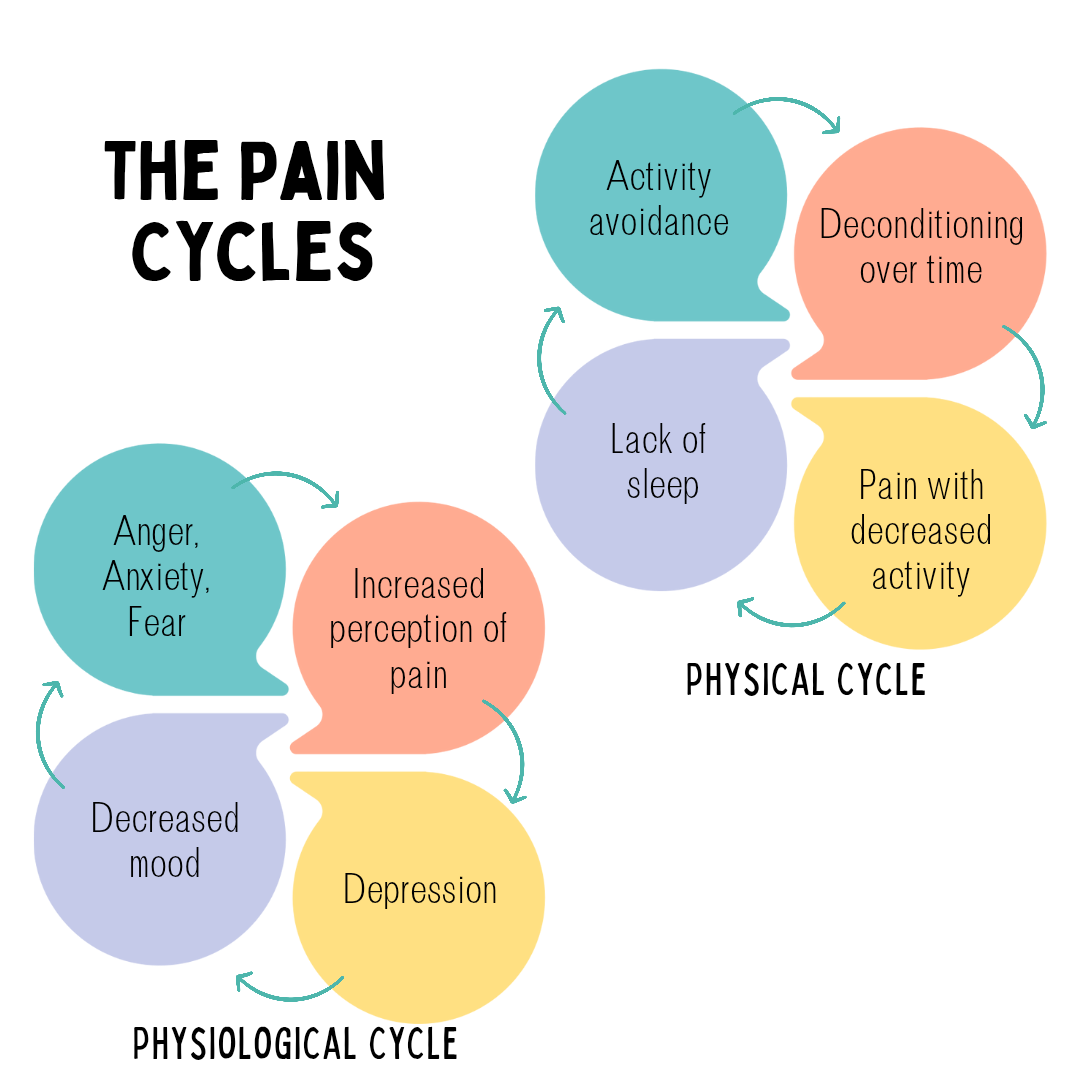
STRESS: I wish this didn't play a role in prolapse but then I would be living under a rock if I didn't believe this. Stress increases prolapse symptoms. This can be both physical stress or emotional stress. We have a section on this later on but a brief overview is that the body works on a fear-->tension-->pain cycle. The more fear we have, the increased tension we have and the more pain we experience. The body is also interconnected so if you typically hold stress in your jaw/TMJ/grind your teeth, there's a good chance you will also experience those sensations in your pelvic floor.
NIGHTTIME: Oftentimes as you are on your feet or constantly on the go, you may notice your prolapse symptoms increase. This is normal because of gravity and fatigue. The normal daily fluctuations are also one reason you can see your doctor and upon evaluation they say you don't have a prolapse but at home (usually at night) you feel more symptoms and maybe even see it. It's not that your doctor or PT is wrong, it's simply that your anatomy changes throughout the day as muscles are used. Over time, with exercise and help, these symptoms usually improve.
CHANGE IN POSITION: Often times when you go to the doctor or pelvic floor rehab provider they will check for prolapse when you are lying on your back with your feet in stirrups or on the table. In this position, it is common that a prolapse may not be present even if you have the symptoms of a prolapse. This is because when we lie down gravity naturally pulls the muscles into a more relaxed state. If you notice a prolapse but your provider hasn't found one, that doesn't mean your lived experience is wrong. It simply means they may not have checked at the right time or correct position. This is one reason later on we will check for a prolapse in different positions, specfically standing up and squatting at these are times you might feel increased prolapse symptoms.

MENSES: 41% of women notice their incontinence is cyclical and of those women 42% notice symptoms just before their period and 36% of women notice increased symptoms during their period. This is commonly for two reasons - the first being hormonal and a decrease in estrogen immediately before menstruation and the second being the position of the uterus as the cervix naturally lowers in the vagina at this time.
While we need more research on cyclical incontinence, it can be helpful to look at the research we do have—specifically increased incontinence during menopause. Menopause, like the premenstrual time frame, is when the natural production of estrogen declines. In fact, estrogen levels are lowest right before, during and immediately after the period. These low estrogen levels can decrease ligament laxity and increase ligament stiffness. What this means is that approximately a week before menses occurs there is a drop in estrogen which is believed to decrease the strength of the urethra, the tube that connects that bladder to the urinary meatus (how we get urine from the bladder to the outside).
The human body is an amazing thing - it changes and adapts to the hormones that our body naturally releases and the pelvic floor is no different. In fact, the pelvic organs as well as the surrounding connective tissues are all estrogen-responsive, meaning the tissues respond and adapt to fluctuations in estrogen. We commonly see this effect in women with stress incontinence who are pre-menopausal due to lower levels of estradiol being produced. With the decrease in estrogen, the pelvic floor and surrounding ligaments are unable to appropriately adapt to changes in intra-abdominal pressure, causing increased incontinence due to the decreased strength, increased stiffness and decreased ligament laxity.
These natural fluctuations in estrogen may also affect the orientation of the cervix. The change in orientation can affect the sphincter of the urethra, or the ability to start/stop the flow of urine efficiently and effectively. This helps us better understand that increased incontinence before and during our periods may be due to the decrease in estrogen which changes the pressure around the urethra causing it to lose elasticity and not being able to fully close and stop the flow of urine.
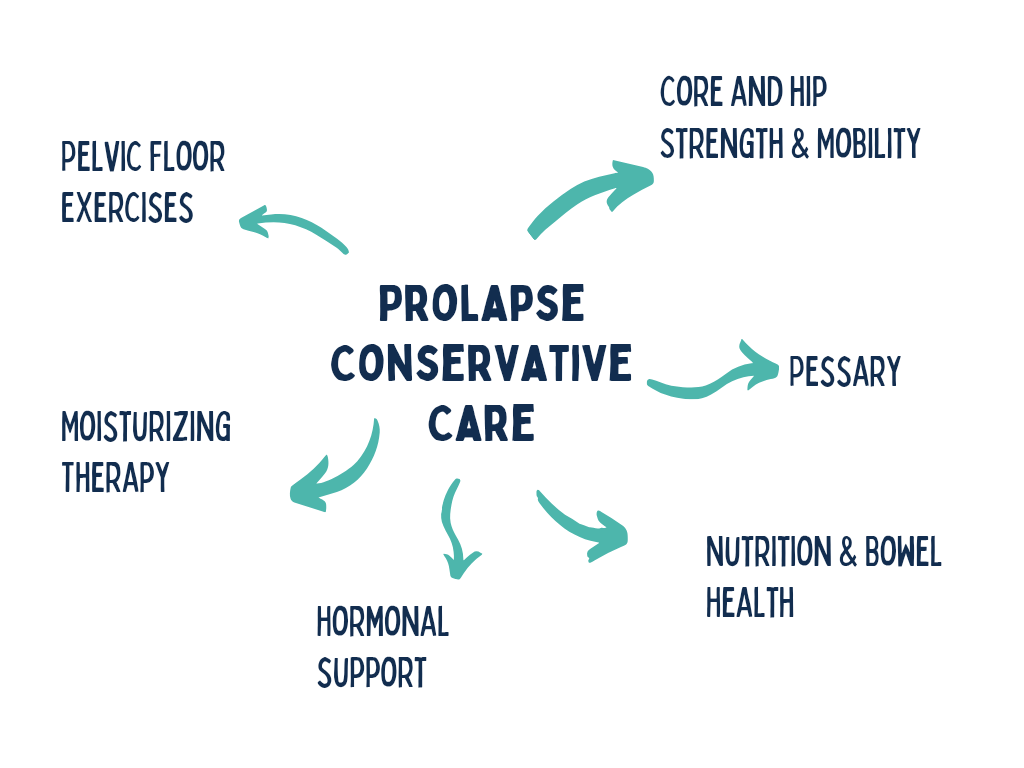
Conservative Pelvic Floor & Prolapse Support
Pelvic Floor Exercises: Research has shown that pelvic floor exercises (kegels) alone can improve 44% of pelvic organ prolapse symptoms and incontinence can improve by 62%.
Exercise: Unfortunately research hasn't looked at core and hip exercises to improve prolapse specifically (yet). What we do know is that strengthening the hips and core has been shown to decrease incontinece.
Nutrition & Bowel Health: Constipation and the increase in bloating and pressure that comes with it has been shown to increase both the grade and symptoms of prolapse.
Pessary: Pessaries are a device you can utilize to physically lift the organs back into place. There are some over-the-counter products like the Poise Impressa or Revive and others need to be fitted by a healthcare professional. Pessaries are a great option to utilize while working on everything else as it keeps the organs nice and lifted and requires less work from the muscles to maintain that support. Similar to riding a bike, it also helps the muscles develop muscle memory so they remember where they should be located!
Estrogen, Hyaluronic Acid, Vitamin E Suppositories: Whether you are looking at topical estrogen or more natural supplements like hyaluronic acid or Vitamin E suppositories, these have all been shown to increase the elasticity of muscle and improve prolapse symptoms.
Supporting your Pelvic Floor Throughout the Day
Now that you know what’s happening down there and how it is connected you might be thinking, “what now?” and that’s totally normal! The good news is that it really depends on you. You know your personality and how you function best.
If you’re the type of person that prefers to dip your toes in the water and you’re not sure if you’re ready to make big changes, that’s okay too! Even small steps each day will get you to your goal. If this is you, think about trying to add these changes one small step at a time - you can start by sitting and standing up from a chair using your entire core whenever you use the restroom or maybe you prefer to do it when you eat meals. Either way, that is still 3-8 more times a day that you are practicing and incorporating the pelvic floor into your daily movement!
If you’re the type of person that needs to jump into the water with both feet - then you can soak in all of this information and look at the attachment below and do everything all at once. You also have permission to slow down and take tiny steps to help you move forward.

Resources to help you move forward
Functional Medicine Provider: Institute for Functional Medicine or Integrative Women’s Health (specialize in women’s health)
Pelvic Floor Rehab Provider: Pelvic Guru or Pelvic Rehab Practitioner
Whole Body Relaxation: Nari Clemons - Meditations for Pelvic Health
Need a little TLC for going to the bathroom? Nari Clemons has a beautiful Toilet Track to help you do just that!