How can acupuncture help with fertility?
Can acupuncture help with hormone imbalances?
Tell me more about acupuncture…is there a special fertility treatment?
Fertility journeys are often full of highs and lows…the emotional rollercoaster of meticulously tracking your cycle, getting excited for ovulation, and the grief that comes when a period begins. Looking at the highs and lows of hormones throughout the cycle, egg count and quality. If you're trying to conceive your body can feel unpredictable, disconnected or maybe you feel downright exhausted.
Fertility isn't *just* about hormones on a lab report. It's about rhythm, regulation and finding balance within the body. This is where acupuncture and Traditional Chinese Medicine (TCM) excel. Balance isn't a scale that's 50/50 and equal. It's ever-changing. It’s a dynamic harmony between yin and yang that fluctuates. It’s the balance of light and dark, hot and cold, movement and rest. It's about meeting your body where it is right now to help bring it into a space of harmony where the body and mind are able to accept life's changes and flow.
Acupuncture Takes a Whole-Person Approach
One reason I love TCM is that everything is connected. You can't separate the body and the mind. Fertility isn't just about the uterus and ovaries. It’s a reflection of how well the entire body is communicating. It looks at:
Sleep quality
Digestive strength and mobility
Emotional regulation
Nervous system
Blood flow quality, quantity and ability to move freely
Cycle flow, color, consistency
Your menstrual cycle isn't just a reproductive event - it's your monthly report card on how well your body is communicating. When you have painful periods, PMDD, infertility, irregular cycles or light/heavy flows, it's your body's way of letting you know it needs more support.
How Does Acupuncture Work?
In TCM we have meridians or pathways that carry energy similar to a sidewalk…connecting everything within a town. Sometimes that sidewalk is too hot and we need to cool it down. Sometimes it's covered in ice and we need to warm the sidewalk to move freely. Sometimes there's a gathering of people that makes it harder to move around the town and we need to disperse the gathering to move freely around town. Acupuncture helps bring balance so the sidewalk system of the body can work smoothly.
From a Western perspective, acupuncture helps:
Improve blood flow to the uterus and ovaries
Regulates the hypothalamic-pituitary-ovarian (HPO) and hypothalamic-pituitary-adren (HPA) axis
Supports hormone signaling
Shifts the nervous system from a sympathetic fight-or-flight to a parasympathetic rest-and-digest
In other words, it helps support the infrastructure of the town so it runs smoothly. In Western medicine, we have generalized labels like infertility, PCOS or luteal phase defect. In Eastern medicine we break that down further by asking WHY. Why is this happening in your body? What patterns do we see that are leading to these labels? Acupuncture looks at the pattern for treatment, not the diagnosis.
Using Acupuncture to Work with Your Cycle
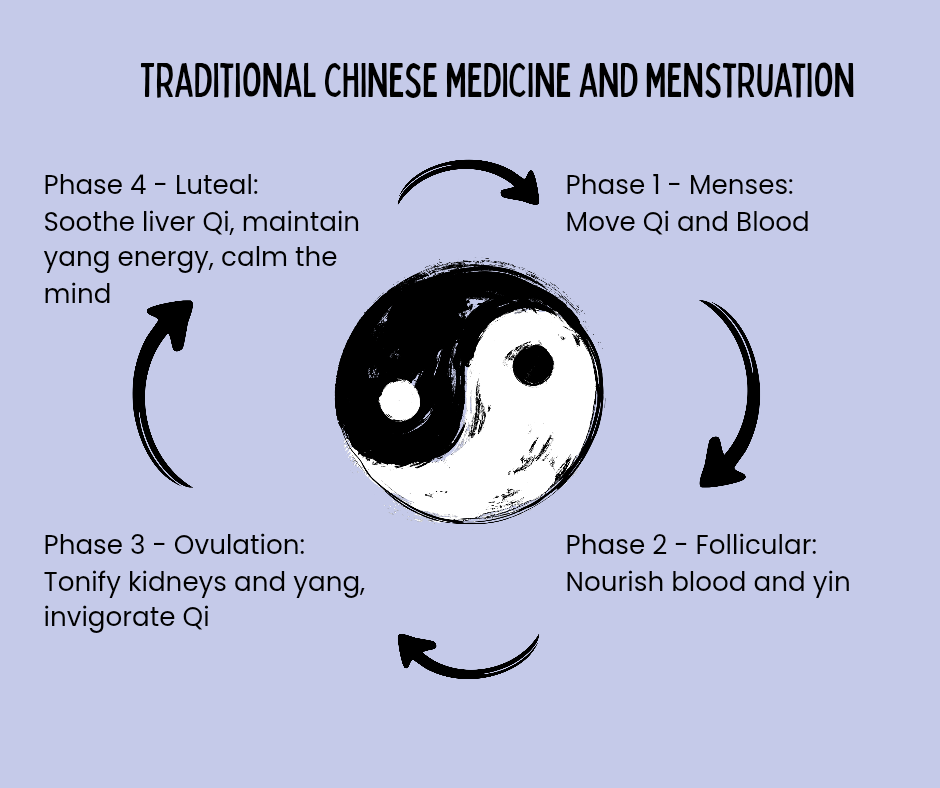
One thing I love about acupuncture for fertility support is how it looks as the cycle as just that, a cycle. It looks at how supporting the body during the bleeding phase can help with the ovulation phase and how ovulation supports the luteal phase and how the luteal phase determines whether we go back to menstruation or into pregnancy. Everything works together.
During the Menstrual phase (Days 1-5/7) is when menstrual bleeding occurs and we have an increase in FSH and LH to stimulate the growth of new follicles/eggs.
In TCM, it's when we focus on resetting and blood movement. It's a time we work on clearing, releasing and improving flow of Qi and blood to make sure the lining of the uterus fully sloughs off.
During the follicular phase (Days 5/7-14/18) is when the ovaries begin to prepare for an egg to be released. It’s when estrogen is increasing and the uterine lining starts to thicken and you have an increase in cervical mucus.
During this phase we focus on building blood and yin. It's a time we work on nourishing the lining and supporting egg development.
During ovulation cervical mucus looks like egg-whites and there is a surge of LH that causes the release of an egg.
We focus on Qi (energy) movement, yin support and communication as the body is releasing a mature egg. It's a time we work on encouraging smooth transitions.
During the luteal phase is when progesterone is the highest as the body thickens the lining of the uterus to get ready for a possible pregnancy.
We focus on warming, and an increase in energy towards the uterus to support a pregnancy. It's the time we support progesterone, implantation and stability.
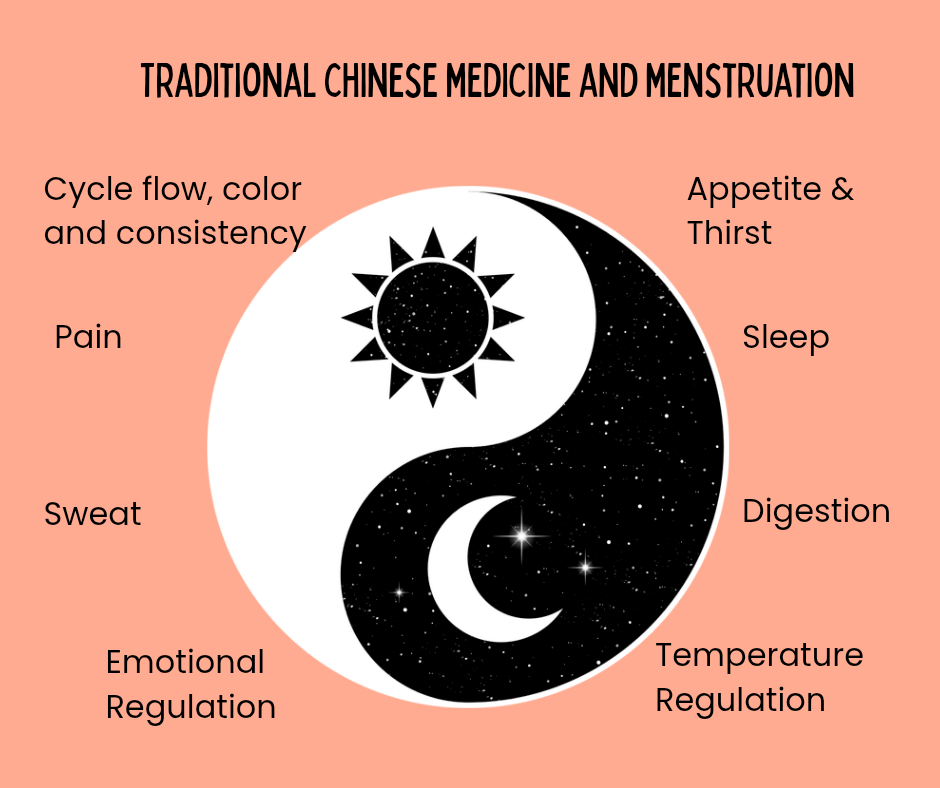
Traditional Chinese Medicine and Menstruation
Acupuncture is just one piece of Traditional Chinese Medicine and it works with your cycle to help bring balance to your body and mind. Fertility can't be forced, it needs to be nourished. In addition to acupuncture needles we also:
Map your cycle patterns - from basal body temperature to mood fluctuations, pain and cervical mucus fluctuations, we want to track it all
Support nervous system regulation - I'm not about to tell you to “just decrease your stress” because in my experience that has never actually worked. What we can do is help you be present and focus on supporting your body and mind right now
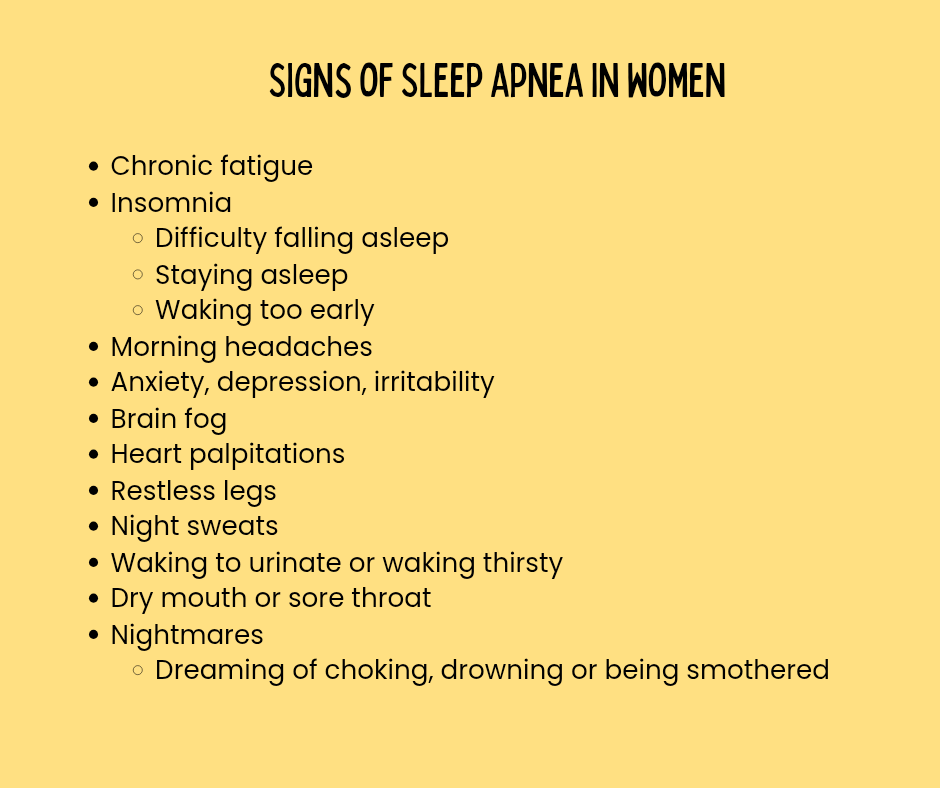
Address sleep issues - whether you struggle to get to sleep, wake frequently, wake at 3am, flop like a fish out of water or never feel rested, it's important to work on sleep which is the time our body naturally heals and nourishes itself
Support digestion - Reflux, constipation, feeling sluggish, all of these are interconnected in TCM. By supporting what and how we eat, we can support digestion and fertility
Menstrual Blood Color and Acupuncture Outlook
Let’s first look at the color of your menstrual blood. A healthy period is typically deep red in color, steady flow (not spotting for a few days before/after period or start/stopping) and free of heavy clots or pain. We're going to take a look at different menstrual blood colors and how they might show up in different TCM patterns.
Bright Red: healthy menstrual blood indicating balance and free flow of Qi (energy) and blood
Dark Red or Brown: Can indicate heat, cold or stagnant blood
If someone has stagnant blood, they frequently feel better if they do gentle exercise right before and during menstruation.
Purple/Maroon: indicated blood stasis or Qi stagnation meaning they blood and Qi aren't able to move freely
There are different forms of stagnation but you may have been diagnosed with PCOS or endometriosis or cysts. You may also notice that you are easily angered or struggle with sleep
Pale/thin/watery: indicates blood or Qi deficiency
If you have thin or watery menstrual blood, you may have noticed a general feeling of fatigue. Or maybe you've noticed that it's nearly impossible to work out during menstruation or right after menses because you are too tired.
Clots: Qi stagnation or cold
If you place the palm of your hand under your belly button, you may notice that it is cold. If this is you, you may have already realized that a hot pad on your lower abdomen or low back helps you feel better.
A Realistic Timeline for Acupuncture
If you check Facebook, you'll notice a wide variety of recommendations. Some people will recommend acupuncture on the day of IVF/IUI transfer. This is a great recommendation because research has shown that it can improve pregnancy rates.
You will also see a lot of people recommend starting acupuncture a minimum of three months before you are TTC or set for an egg retrieval. This is because it takes roughly 90-120 days for a human egg to mature from its dormant state to immature state to being ready for ovulation. The changes you make today will help fully support the egg you are ovulating in three months.
While I prefer to work with people for three to four months prior to retrieval or TTC, I know that isn't financially realistic for everyone. The thought of “another appointment” can also increase stress for some. If that's you, it's important to talk to your acupuncture provider to find a balance that works for you! You don't need a plan that stresses you out. You need a regulated, supported and understood system. And that's exactly what we can do together.